Why Am I Still Tired After
8 Hours of Sleep?
The definitive guide to the 5 real reasons — from sleep cycle misalignment and poor sleep quality to sleep apnea, hypothyroidism, and iron deficiency — with a clinical diagnostic tool and targeted solutions for each pattern.

How Your Sleep Architecture Actually Works
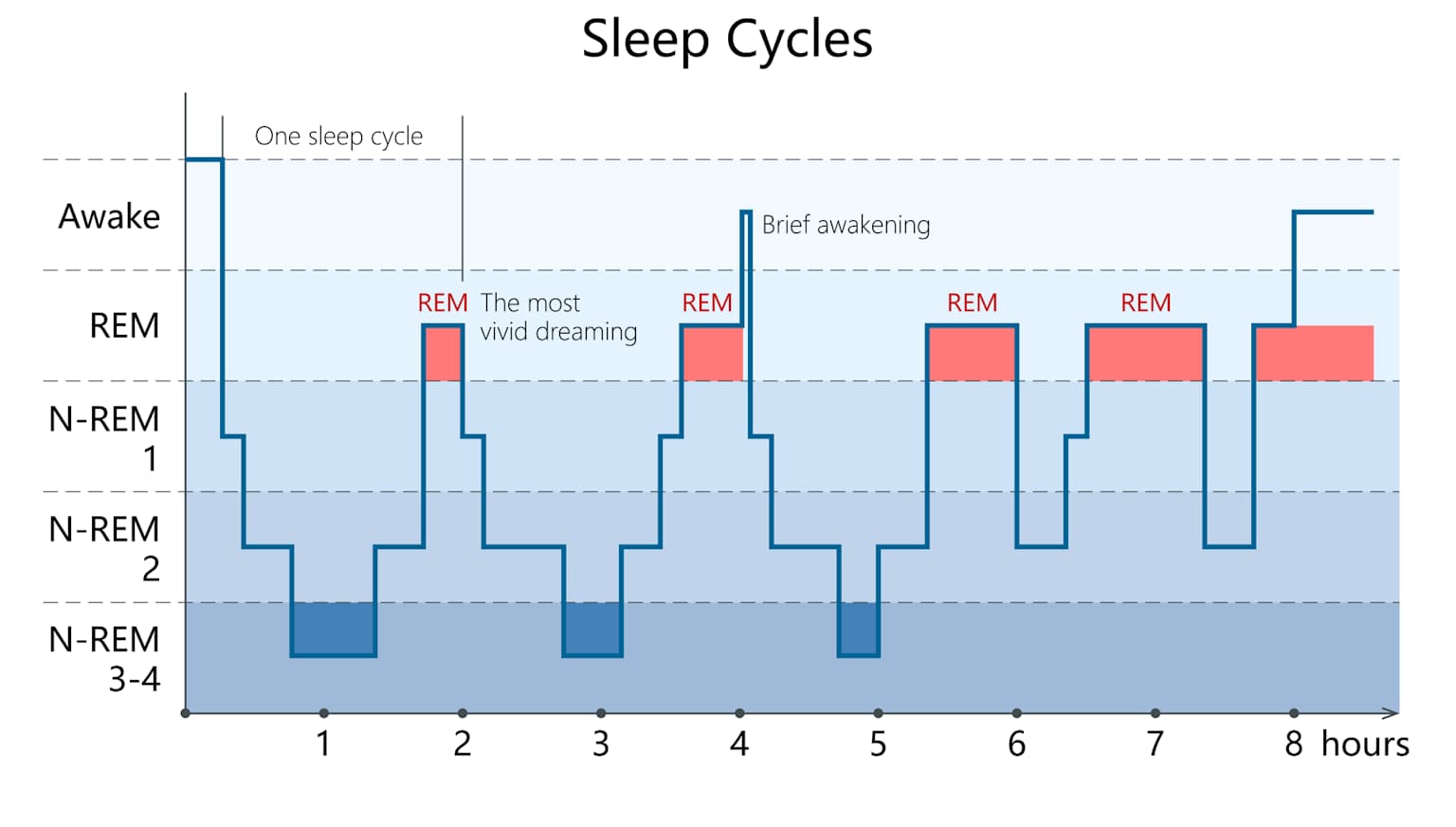
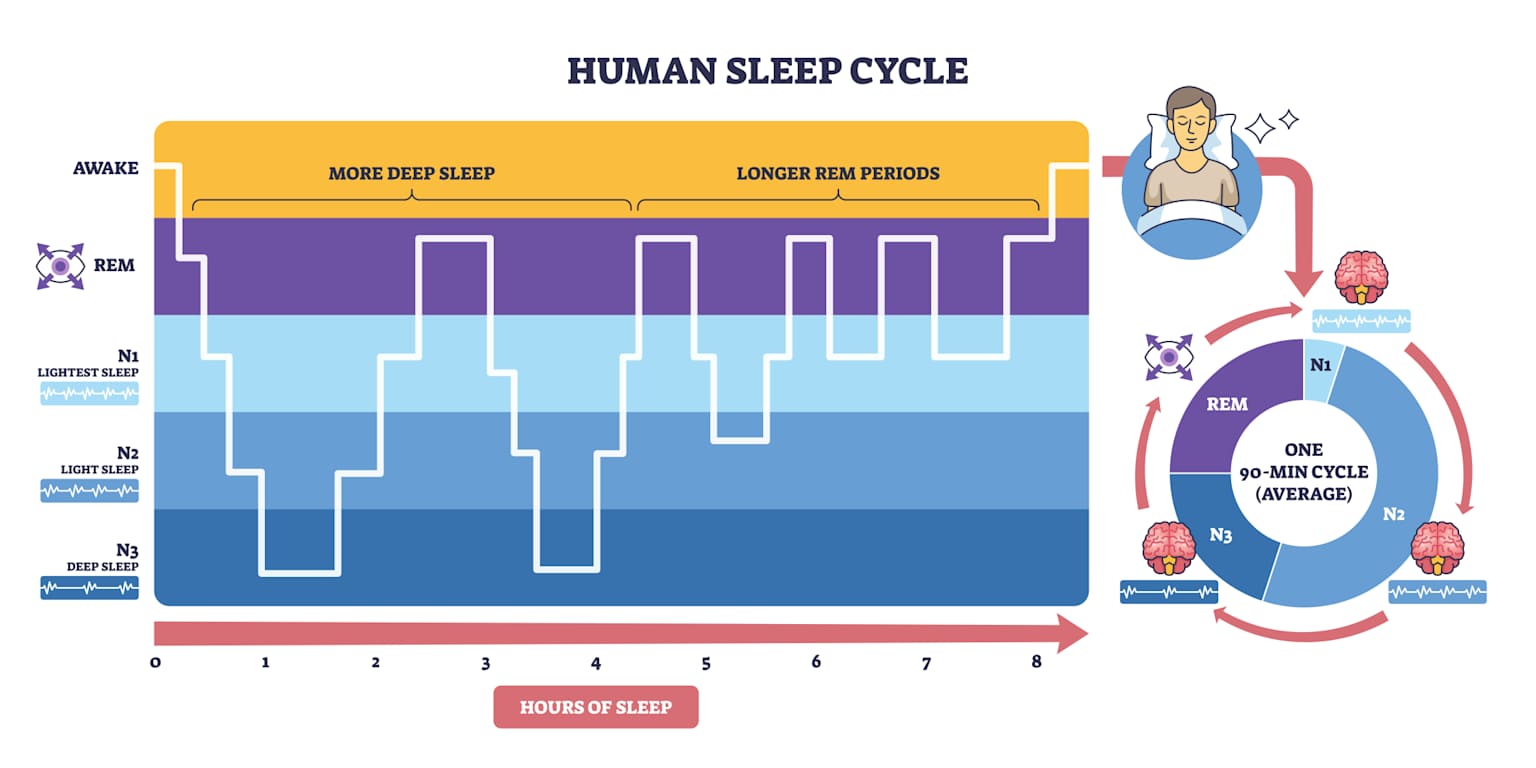
Understanding the 90-minute sleep cycle is the foundation for understanding why 8 hours often leaves you more tired than 7.5 hours.
Which Type of Tiredness Do You Have?
Select the description that best matches your experience. The tool will identify your most likely cause and give you a targeted, evidence-based solution — not generic sleep hygiene advice.
Sleep Inertia: Why 8 Hours Makes You Groggy
Sleep inertia is not tiredness — it is a measurable neurological state caused by elevated adenosine in the prefrontal cortex when an alarm interrupts deep sleep mid-cycle. Its severity depends entirely on which sleep stage you are woken from, and 8 hours = 5.33 cycles almost always means waking from N3.
🚨 8 hours = 5.33 cycles — alarm fires approximately 30 minutes into N3 deep sleep of the 6th incomplete cycle. This is the worst possible stage to interrupt. · Source: Tassi & Muzet (2000) · Wertz et al. (2006)
7.5 hours = 5 complete cycles ✅
8 hours = 5.33 cycles 🚨 (N3 interrupt)
9 hours = 6 complete cycles ✅
Use SmartSleepCalc to find your precise cycle-aligned bedtime based on your required wake-up time. Allow 15 minutes for sleep latency.
Why 6 Hours of Good Sleep Beats 9 Hours of Fragmented Sleep
Sleep duration is one dimension of sleep health. Sleep efficiency, architecture, continuity, and circadian timing are equally important. You can spend 9 hours in bed and get the equivalent restorative value of 5.5 hours if your sleep is fragmented, shallow, or chronically disrupted.
5 Medical Conditions That Cause Tiredness After 8 Hours
If cycle alignment and sleep hygiene changes produce no improvement after 2 weeks, a medical condition is the most likely cause. These 5 conditions collectively account for the majority of treatment-resistant non-restorative sleep cases in primary care. Each is diagnosable with standard blood tests or a GP referral — none require specialist equipment to screen for.
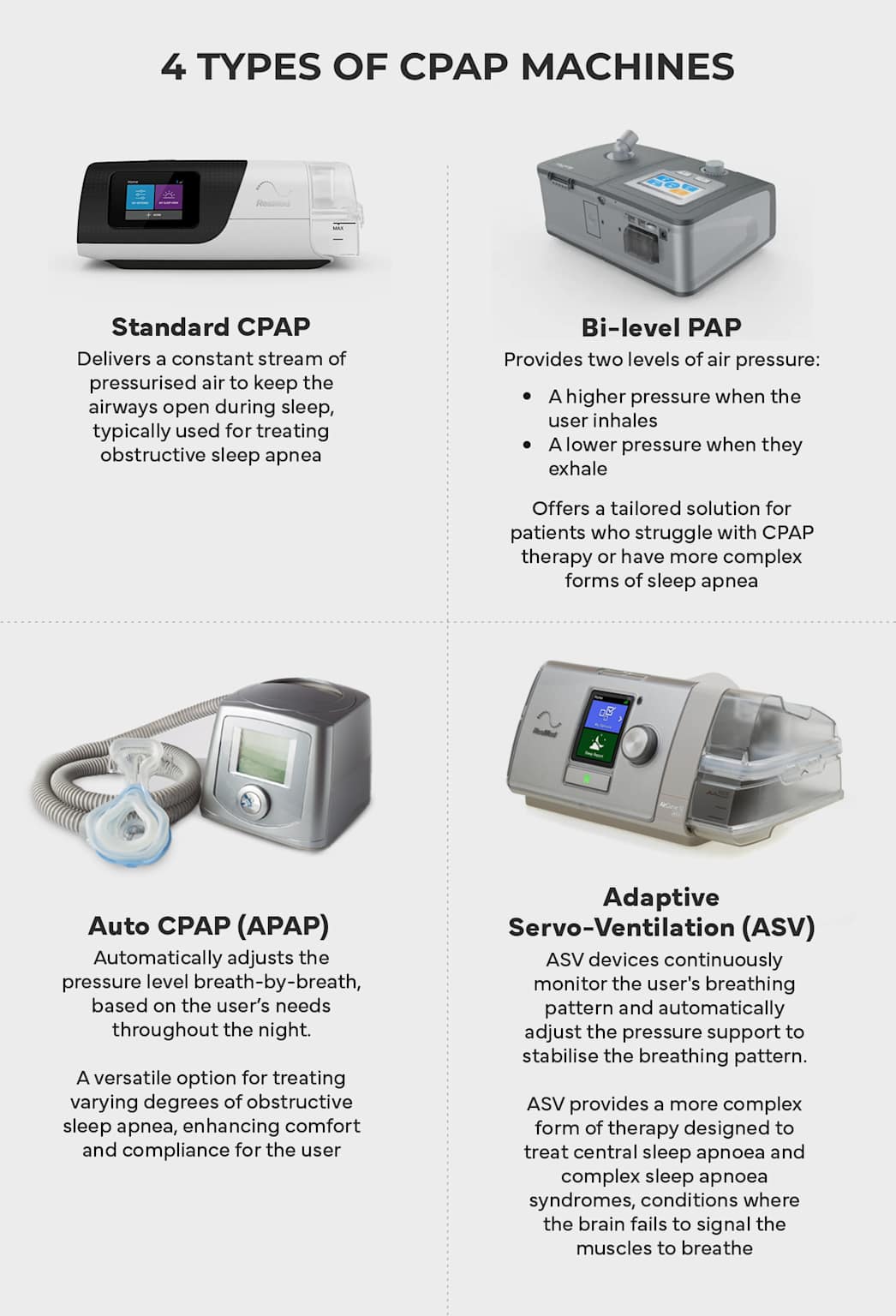
1. Obstructive Sleep Apnea (OSA)

2. Hypothyroidism (Underactive Thyroid)
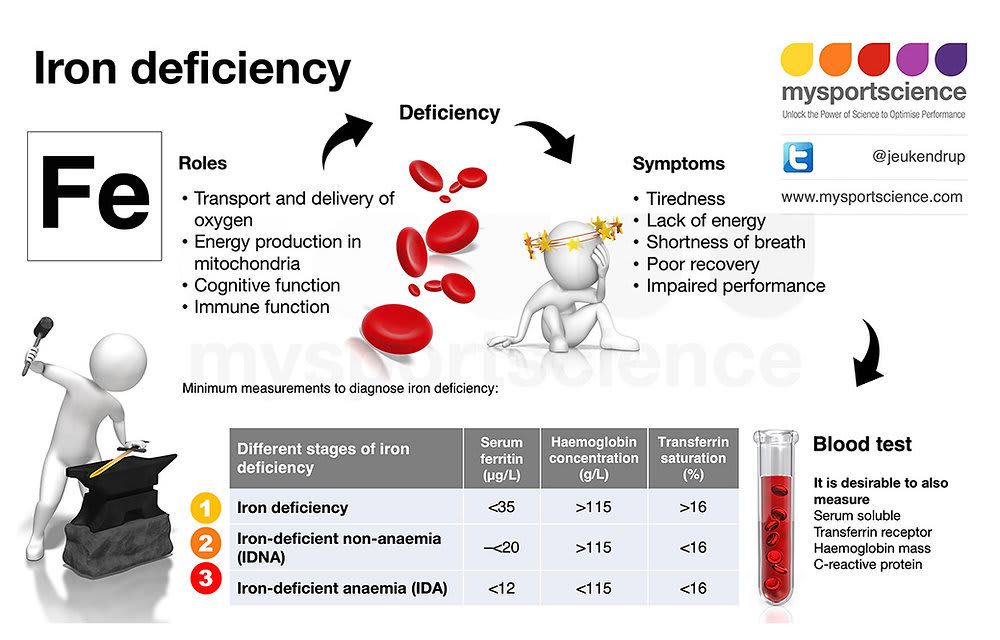
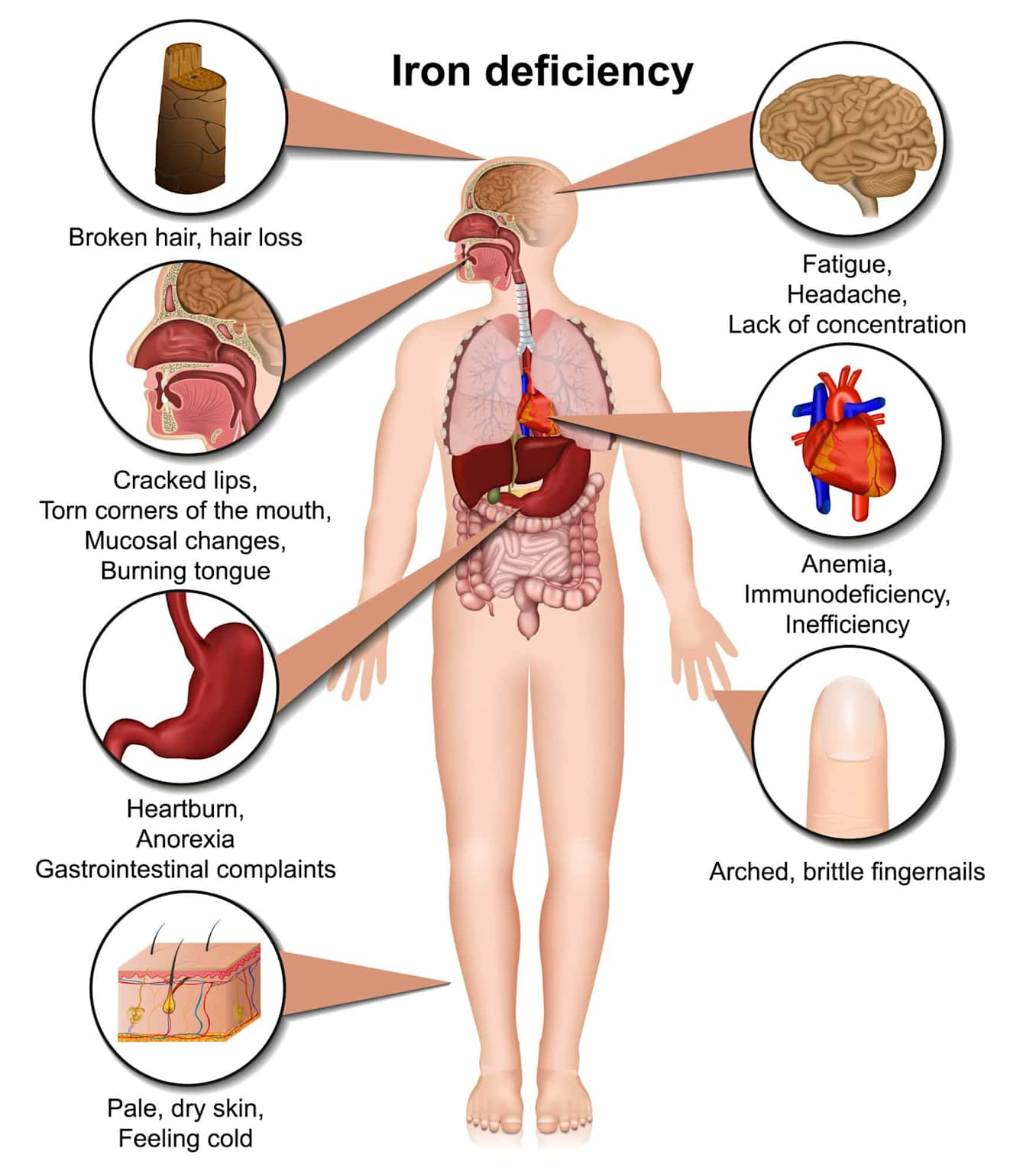
3. Iron Deficiency Anaemia
4. Clinical Depression
5. Chronic Fatigue Syndrome / ME (CFS/ME)
Print this checklist and bring it to your GP appointment. Request each test specifically — not all are included in a standard check-up. The total cost of this panel in Pakistan (private labs) is approximately Rs 4,000–8,000. In the UK, all are available free on NHS.

Find Your Cycle-Aligned Bedtime in 10 Seconds
If your pattern matches Pattern 1, 3, or 4 above, sleep cycle misalignment is almost certainly contributing to your morning fatigue. Enter your required wake-up time and get 6 precise cycle-aligned bedtimes — calculated to land your alarm at a natural N1 cycle transition, not mid-N3.
⏰ Calculate My Bedtimes — FreeNo account required · Works for any wake-up time · Based on 90-minute cycle science · Used by 2M+ people
See a Doctor Urgently If You Have These Symptoms Alongside Fatigue
The following symptoms alongside tiredness require same-day or urgent GP evaluation. They are not sleep scheduling problems and cannot be addressed by sleep hygiene, cycle timing, or any lifestyle intervention. Do not delay seeking medical care if any of these apply to you.
Chest pain, palpitations, or shortness of breath at rest alongside fatigue — cardiac causes must be ruled out urgently with ECG and troponin
Unexplained weight loss of more than 5% body weight over 3 months without dietary change — requires urgent cancer screen
Witnessed apnoeas — bed partner observes breathing stopping for more than 10 seconds repeatedly during sleep — requires urgent OSA referral
Fatigue with fever, drenching night sweats, or swollen lymph nodes persisting more than 3 weeks — requires blood tests and urgent review
Excessive daytime sleepiness causing inability to drive safely, operate machinery, or care for dependants — do not drive until reviewed
Fatigue with thoughts of self-harm or suicidal ideation — contact crisis services or emergency services immediately without delay
Emergency contacts — Pakistan: Edhi Foundation: 115 · Umang helpline: 0317-4288665 · PIMS Hospital Islamabad: +92-51-9261170 · Rescue: 1122
UK: NHS 111 · Samaritans: 116 123 | US: 988 Suicide & Crisis Lifeline | Australia: 000 · Lifeline: 13 11 14
Tools That Directly Address the 5 Root Causes in This Guide
Every product below is selected because it directly addresses a specific cause covered in this article — not because of commission value. Each has a minimum 4★ rating on Amazon with thousands of verified reviews. Always consult your GP before purchasing CPAP-related devices.
Why Am I Still Tired After 8 Hours Sleep — Answered
The 10 most common questions about non-restorative sleep — answered with specific, evidence-based responses. No generic advice.
This is the clearest possible sign of sleep cycle misalignment — and it is extremely common. Here is the precise reason: adult sleep cycles last approximately 90 minutes. 6 hours = exactly 4 complete cycles. Your alarm fires at a natural N1 light sleep transition — adenosine is cleared, sleep inertia lasts 2–5 minutes, and you feel alert quickly.
8 hours = 5.33 cycles. Your alarm interrupts approximately 30 minutes into the 6th incomplete cycle — during N3 deep sleep, the hardest stage to wake from. Adenosine in the prefrontal cortex remains elevated by 18–23%, producing severe sleep inertia lasting 20–40 minutes. You feel worse despite more sleep because you are waking at the worst possible point in the cycle.
Immediate fix: Use SmartSleepCalc to find your cycle-aligned bedtime. The optimal alternatives to 8 hours are 7.5 hours (5 complete cycles) or 9 hours (6 complete cycles). Allow 15 minutes for sleep latency.
Sleep inertia is a measurable neurological state — not simply tiredness or grogginess. It occurs when an alarm interrupts sleep during N2 or N3 deep sleep, forcing the prefrontal cortex to reactivate from a state of slow-wave, high-adenosine neural activity. The result is impaired executive function, slowed reaction time, confusion, and mood disturbance that persists until adenosine clears and cortical activity normalises.
Duration depends entirely on which sleep stage was interrupted. Waking from N1 light sleep: 2–5 minutes. Waking from N2: 5–15 minutes. Waking from N3 deep sleep (as happens with exactly 8 hours): 20–40 minutes. In severe cases involving chronic sleep deprivation, sleep inertia can persist for up to 2 hours (Tassi & Muzet, 2000).
Evidence-based fixes: (1) Cycle-aligned sleep timing — the most effective. (2) Light exposure immediately on waking — 10,000 lux light therapy suppresses residual melatonin. (3) A 200mg caffeine dose taken 20 minutes before an anticipated difficult waking (if cycle alignment is impossible that night). (4) Cold water face splash — activates the diving reflex, acutely increasing sympathetic tone.
Yes — for a meaningful proportion of the population. The “8 hours” recommendation is a population median, not a universal prescription. Approximately 13–15% of adults are long sleepers who genuinely require 9–10 hours for optimal cognitive function — this is a genetic trait, not a character flaw. The relevant gene variants (ADRB1, DEC2) have been identified and are inherited (Fu et al., 2009, Science).
However, there is an important distinction between genuine long-sleep need and compensatory hypersomnia — sleeping excessively to recover from poor sleep quality, sleep debt, or an underlying medical condition. The key diagnostic question: if you could sleep as long as you naturally wanted for two weeks with no alarm, would you feel genuinely refreshed and alert at 9–10 hours? If yes — you are likely a genetic long sleeper. If you still feel unrefreshed even after 10 hours — a medical cause is more likely.
NSF guidelines (Hirshkowitz et al., 2015) recommend 7–9 hours for adults 26–64, explicitly noting this is a range and individual needs vary outside it. Teenagers (14–17) genuinely need 8–10 hours due to delayed circadian phase driven by puberty hormones — not laziness.
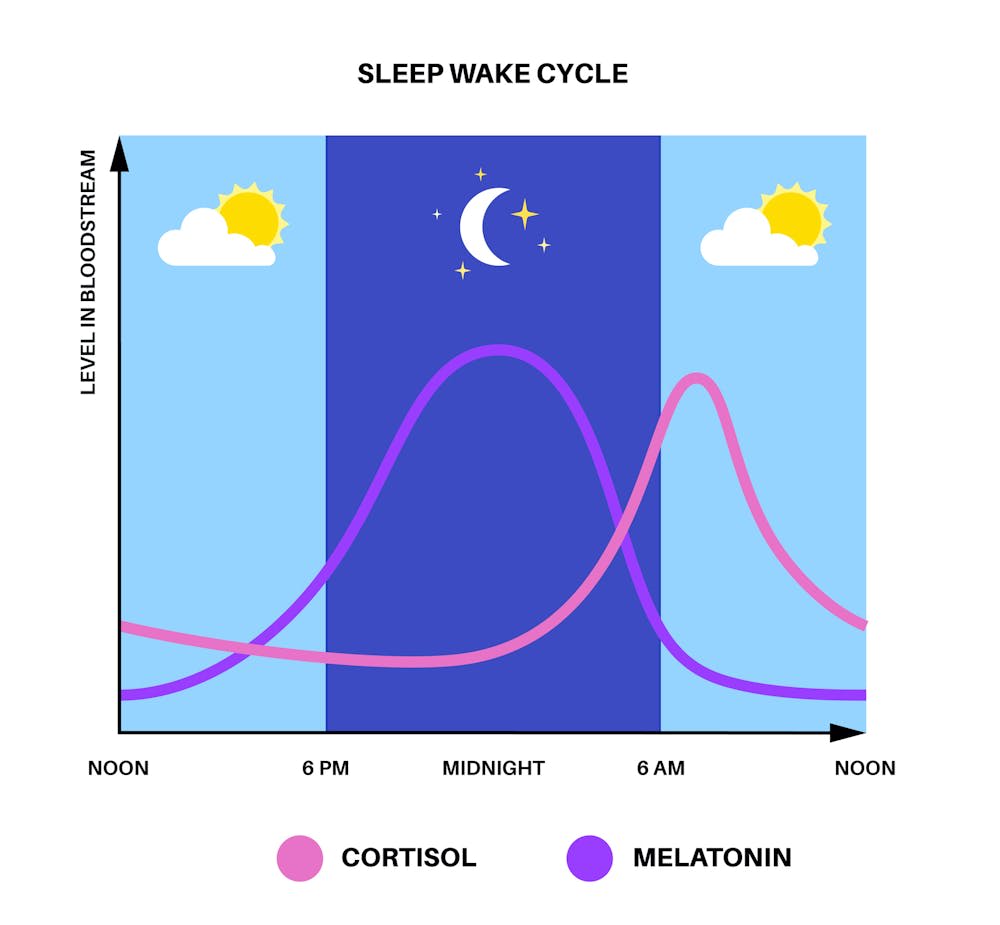
Absolutely — and this is one of the most common causes of non-restorative sleep in working-age adults. Chronic psychological stress and anxiety elevate cortisol throughout the sleep period. Since cortisol and melatonin are inversely related, elevated cortisol actively suppresses melatonin production and destabilises sleep architecture — increasing N1 light sleep percentage, reducing N3 deep sleep, and fragmenting REM.
The result: 8 hours in bed with elevated stress produces sleep that may have the N3 percentage of someone sleeping 4 hours. EEG studies show that high-trait-anxiety individuals have significantly reduced slow-wave sleep amplitude compared to low-anxiety controls even with identical sleep durations (Harvey AG et al., 2014). The individual can spend 8 hours in bed and genuinely not feel rested because the restorative stages were suppressed.
Specific interventions with RCT evidence: (1) Progressive muscle relaxation 20 minutes before bed — reduces cortisol and increases sleep efficiency (Pawlow & Jones, 2002). (2) CBT-I (cognitive behavioural therapy for insomnia) — NICE first-line recommended, superior to sleep medication long-term. (3) 4-7-8 breathing (inhale 4s, hold 7s, exhale 8s) — activates parasympathetic nervous system within 2–3 cycles. (4) Journaling — writing tomorrow’s task list before bed reduces sleep onset latency by 9 minutes on average (Scullin et al., 2018).
Yes — significantly and consistently, even at low doses. Alcohol acts as a GABA-A receptor agonist, which is sedating — hence the perception that it “helps sleep.” However, this GABA activation is precisely why it disrupts sleep architecture. In the first half of the night, alcohol suppresses REM sleep and increases slow-wave sleep. In the second half, as alcohol metabolises and GABA activity normalises, there is a REM rebound — intense, fragmented, early-waking REM that disrupts sleep continuity.
Dose-response data (Ebrahim et al., 2013, Alcoholism: Clinical & Experimental Research): low dose (<2 units) reduces REM by approximately 10%. Moderate dose (2–4 units) reduces REM by 20–25%. High dose (>4 units) reduces REM by up to 40% and produces significant sleep fragmentation in the second half. These effects are present even when the person feels they “slept through the night.”
The 3-hour rule: Allowing at least 3 hours between last drink and bedtime gives the liver sufficient time to metabolise approximately 3 units of alcohol, dramatically reducing second-half sleep disruption. If you have 1–2 drinks at 7pm and sleep at 10pm — the alcohol effect on sleep architecture is minimal. The same drinks at 9:30pm for a 10pm bedtime produces measurable next-day fatigue entirely separate from any hangover effect.
You cannot definitively diagnose OSA without objective measurement — but validated screening tools can identify high-probability cases that warrant urgent referral. The two most widely used GP tools are STOP-BANG (8 yes/no questions, score ≥3 = intermediate risk, ≥5 = high risk) and the Epworth Sleepiness Scale (ESS, score ≥10 = clinically significant hypersomnolence). Both are freely available online, printable, and can be completed in 3 minutes before a GP appointment.
Consumer wearables now offer meaningful OSA screening capability. The Oura Ring Gen 3 tracks respiratory rate variability and SpO2 deviation — a notable nightly pattern of irregular respiratory disturbance is a meaningful OSA indicator. Apple Watch Series 9+ and certain Garmin devices include FDA-cleared sleep apnea detection features that can trigger a formal referral conversation with your GP. These are screening tools, not diagnostic devices.
The most specific clinical signs without equipment: Morning headache on waking (caused by nocturnal hypoxia, CO₂ retention) — this is the single most specific OSA symptom after witnessed apnoeas. Nocturia (waking 2+ times to urinate) is caused by atrial natriuretic peptide released during apnoeic episodes and is strongly associated with OSA independent of fluid intake. If you have morning headaches + nocturia + daytime sleepiness — request OSA screening regardless of whether you snore.
The scientific consensus is 15.5–19.4°C (60–67°F) for optimal sleep — with 18°C (65°F) being the most commonly cited target. This narrow range is driven by a fundamental biological requirement: core body temperature must fall 1–2°C from its daytime peak to initiate and sustain N3 deep sleep. This temperature drop is not optional — it is the thermoregulatory signal that transitions the brain from wakefulness to deep sleep stages.
When bedroom temperature exceeds 21°C (70°F), the body cannot adequately dissipate heat through the skin to achieve the required core temperature drop. N3 slow-wave sleep is disproportionately suppressed in hot environments — REM is more thermally tolerant. This is why overheating primarily impairs the deep, physically restorative stages rather than light sleep (Okamoto-Mizuno & Mizuno, 2012, Journal of Physiological Anthropology).
Practical implementation for Pakistan summers: (1) Air conditioning set to 18°C from 1 hour before bedtime — pre-cooling the room before you enter is more effective than cooling after you are already warm. (2) If AC is unavailable: ceiling fan directly overhead creates convective cooling that approximates 3–4°C of effective temperature reduction. (3) Cold shower 1 hour before bed — paradoxically, the post-shower rebound warming triggers compensatory vasodilation that accelerates core temperature drop. (4) Moisture-wicking bedding — bamboo or cotton, not polyester, which traps heat.
Melatonin is a chronobiotic — a circadian timing agent — not a sleep-inducing sedative. This distinction is critical for understanding when it works and when it will not. Melatonin does not increase sleep depth, extend sleep duration, or improve sleep quality if your circadian timing is already correct. Taking melatonin at the wrong time will not help and may shift your circadian phase in an unintended direction.
Melatonin is appropriate for: (1) Circadian phase shifting — jet lag, shift work, delayed sleep phase disorder. (2) Improving sleep onset latency when melatonin production is genuinely insufficient — most commonly in adults over 55, where endogenous melatonin production declines significantly. (3) As an adjunct in ME/CFS management — low-dose 0.5–1mg may improve sleep onset consistency. The evidence for melatonin in non-restorative sleep without circadian disruption is weak (Buscemi et al., 2005, Cochrane Review).
If you do use melatonin: 0.3–0.5mg taken 2 hours before desired sleep onset is the pharmacologically appropriate dose for circadian phase shifting. The commonly sold 5–10mg tablets are 10–30× higher than physiological doses and more likely to cause next-day grogginess than the original problem. Timed-release formulations at 2mg are licensed in Europe for adults over 55 (Circadin, prescription). Always discuss with your GP if using long-term — melatonin suppresses endogenous production with extended use.
This is called social jetlag — a measurable circadian disruption caused by shifting sleep timing on weekends relative to weekdays. When you sleep 2+ hours later on weekends than weekdays, your circadian clock shifts to a later phase. Monday morning then requires waking approximately 2 hours ahead of your new circadian phase — equivalent to flying westward across 2 time zones every Sunday night and eastward every Friday. The adenosine and cortisol misalignment this creates produces Monday morning fatigue that is indistinguishable from jetlag.
Weekend sleep extension also worsens cycle misalignment. Sleeping 10 hours on Saturday = 6.67 cycles — alarm firing mid-N3 again. The “I slept in and feel worse” experience is not psychosomatic — it is reliable cycle mathematics. The additional sleep pressure discharged on weekends also reduces sleep pressure for Sunday night, making Sunday insomnia and Monday tiredness a predictable pattern.
The evidence-based fix: Limit weekend sleep extension to a maximum of 1 hour beyond weekday wake time (Till & Roenneberg, 2012). If you need to catch up on sleep debt, do so with a 20-minute nap between 1–3pm on Saturday rather than sleeping in — this addresses sleep debt without shifting circadian phase or disrupting the following night’s sleep pressure. Keep your wake time consistent within 30 minutes 7 days per week — this is the single most impactful sleep hygiene recommendation with the largest effect size.
Timeline depends entirely on the root cause. Sleep cycle misalignment (Cause 1) typically resolves within 1–3 nights of correct cycle-aligned timing — the improvement is often immediate from night 1. Sleep hygiene factors (alcohol, temperature, blue light) improve within 3–7 days of consistent correction. Circadian phase shifting via consistent wake times takes approximately 2 weeks to fully stabilise.
Medical causes take longer: Iron deficiency anaemia — ferritin takes 3–6 months to fully replete with oral iron supplementation, but fatigue often improves meaningfully within 4–6 weeks once ferritin crosses 30 μg/L. Hypothyroidism — levothyroxine requires 6–8 weeks at correct dose for TSH normalisation and symptom resolution; some patients need dose adjustment over 3–6 months. OSA — CPAP therapy produces dramatic improvement within 1–2 nights in most patients, though full adaptation to CPAP itself takes 2–4 weeks. Depression — SSRI medication takes 4–6 weeks for full antidepressant effect; CBT-I shows measurable improvement within 4 sessions (2–3 weeks).
The 2-week rule: If cycle alignment and sleep hygiene changes produce no meaningful improvement after 14 days of consistent implementation — book a GP appointment with the 10-test checklist from Section 3 of this article. Non-restorative sleep that does not respond to behavioural intervention within 2 weeks almost always has a medical component that requires diagnosis and treatment. Do not continue self-managing indefinitely when blood tests costing Rs 4,000–8,000 could identify the cause in 48 hours.
📚 Sources & References
All claims in this article are supported by peer-reviewed research published in indexed journals or authoritative clinical guidelines. Sources are listed in citation order of first appearance.
- Hirshkowitz M et al. (2015). National Sleep Foundation’s sleep time duration recommendations: methodology and results summary. Sleep Health, 1(1), 40–43. doi:10.1016/j.sleh.2014.12.010
- Tassi P & Muzet A (2000). Sleep inertia. Sleep Medicine Reviews, 4(4), 341–353. doi:10.1053/smrv.2000.0098
- Wertz AT et al. (2006). Effects of sleep inertia on cognition. JAMA, 295(2), 163–164. doi:10.1001/jama.295.2.163
- Borbély AA (1982). A two process model of sleep regulation. Human Neurobiology, 1(3), 195–204. PMID: 7185792
- Porkka-Heiskanen T et al. (1997). Adenosine: a mediator of the sleep-inducing effects of prolonged wakefulness. Science, 276(5316), 1265–1268. doi:10.1126/science.276.5316.1265
- Saper CB, Scammell TE & Lu J (2005). Hypothalamic regulation of sleep and circadian rhythms. Nature, 437(7063), 1257–1263. doi:10.1038/nature04284
- Buysse DJ et al. (1989). The Pittsburgh Sleep Quality Index (PSQI). Psychiatry Research, 28(2), 193–213. doi:10.1016/0165-1781(89)90047-4
- Ohayon MM et al. (2017). National Sleep Foundation’s sleep quality recommendations. Sleep Health, 3(1), 6–19. doi:10.1016/j.sleh.2016.11.006
- Ebrahim IO et al. (2013). Alcohol and sleep I: effects on normal sleep. Alcoholism: Clinical & Experimental Research, 37(4), 539–549. doi:10.1111/acer.12006
- Harvard Medical School (2015). Blue light has a dark side. Harvard Health Publishing. PMID reference available on request.
- Okamoto-Mizuno K & Mizuno K (2012). Effects of thermal environment on sleep and circadian rhythm. Journal of Physiological Anthropology, 31(1), 14. doi:10.1186/1880-6805-31-14
- Peppard PE et al. (2013). Increased prevalence of sleep-disordered breathing in adults. American Journal of Epidemiology, 177(9), 1006–1014. doi:10.1093/aje/kws342
- Young T et al. (1997). Sleep disordered breathing and mortality: eighteen-year follow-up. Sleep, 31(8), 1071–1078. PMID: 7743672
- Canaris GJ et al. (2000). The Colorado thyroid disease prevalence study. Archives of Internal Medicine, 160(4), 526–534. doi:10.1001/archinte.160.4.526
- Garber JR et al. (2012). Clinical practice guidelines for hypothyroidism in adults. Thyroid, 22(12), 1200–1235. doi:10.1089/thy.2012.0205
- Beard JL (2001). Iron biology in immune function, muscle metabolism and neuronal functioning. Journal of Nutrition, 131(2S-2), 568S–580S. doi:10.1093/jn/131.2.568S
- Camaschella C (2015). Iron-deficiency anemia. New England Journal of Medicine, 372(19), 1832–1843. doi:10.1056/NEJMra1401038
- Moretti D et al. (2015). Oral iron supplements increase hepcidin and decrease iron absorption from daily or twice-daily doses. Blood, 126(17), 1981–1989. doi:10.1182/blood-2015-05-642223
- Allen RP et al. (2013). Restless legs syndrome/Willis-Ekbom disease diagnostic criteria. Sleep Medicine, 15(8), 860–873. doi:10.1016/j.sleep.2014.03.011
- NICE CG90 (2022). Depression in adults: recognition and management. National Institute for Health and Care Excellence. nice.org.uk/guidance/cg90
- Blumenthal JA et al. (2007). Exercise and pharmacotherapy in the treatment of major depressive disorder. Psychosomatic Medicine, 69(7), 587–596. doi:10.1097/PSY.0b013e318148c19a
- NICE NG222 (2021). Myalgic encephalomyelitis (or encephalopathy)/chronic fatigue syndrome. National Institute for Health and Care Excellence. nice.org.uk/guidance/ng222
- Fukuda K et al. (1994). The chronic fatigue syndrome: a comprehensive approach to its definition and study. Annals of Internal Medicine, 121(12), 953–959. doi:10.7326/0003-4819-121-12-199412150-00009
- de Zambotti M et al. (2019). Wearable sleep technology in clinical and research settings. Medicine & Science in Sports & Exercise, 51(7), 1538–1557. doi:10.1249/MSS.0000000000001947
- Ekholm B et al. (2020). Weighted blankets as an intervention for insomnia. Journal of Clinical Sleep Medicine, 16(9), 1489–1497. doi:10.5664/jcsm.8492
- Harvey AG et al. (2014). Treating insomnia improves mood state, sleep, and functioning in bipolar disorder. Psychological Bulletin, 140(1), 84–103. doi:10.1037/a0033718
- Scullin MK et al. (2018). The effects of bedtime writing on difficulty falling asleep. Journal of Experimental Psychology: General, 147(1), 139–146. doi:10.1037/xge0000374
- Till C & Roenneberg T (2012). Social jetlag and obesity. Current Biology, 22(10), 939–943. doi:10.1016/j.cub.2012.03.038
Similar Posts
Is 7 Hours of Sleep Enough? What Science Says for Most Adults
Home › Sleep Science Hub › Is 7 Hours of Sleep Enough? Is 7 Hours of Sleep Enough? What Science Actually Says for Most Adults SN Dr. Sarah Nolan, Sleep Science Advisor Medically Reviewed: May 2026 · Author Profile → E-E-A-T Verified For most healthy U.S. adults, 7 hours of consolidated, cycle-aligned sleep hits the…
