Body Temperature During Sleep: The Overnight Curve, Stage-by-Stage Data & Warm Bath Protocol
Your core body temperature does not stay constant during sleep. It follows a precise circadian trajectory — falling up to 1.0°C through the night, reaching its nadir around 2am, then rising again toward waking. This overnight drop is not a consequence of sleep — it is a prerequisite for it, and it drives the architecture of every sleep stage you pass through.
The Overnight Core Temperature Curve
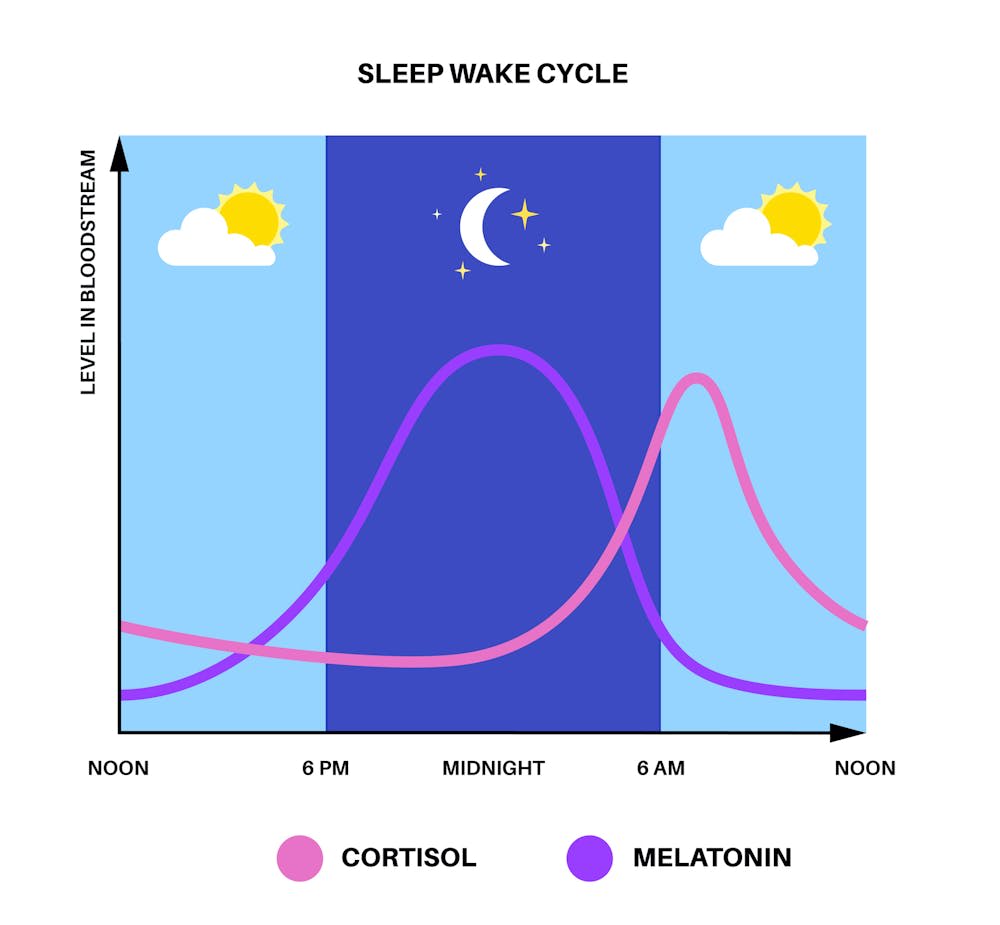
Core body temperature peaks in the late afternoon — approximately 37.0–37.2°C — and begins a sustained decline around 9pm, driven by the circadian pacemaker in the suprachiasmatic nucleus and rising melatonin secretion. Heat is dissipated through vasodilation of skin blood vessels — which is why your hands and feet warm up before bed. The lowest point (the nadir) occurs around 2am, after which temperature gradually rises through the morning under the influence of the cortisol awakening response.
📊 Core Body Temperature Trajectory Across Sleep — Typical Healthy Adult
Data represents a typical healthy adult pattern. Individual variation is significant — chronotype (morning lark vs night owl) shifts the entire curve by 1–2 hours in either direction. Athletes show a deeper nadir due to superior cardiovascular heat dissipation capacity. Source: Kräuchi K et al., Sleep and Circadian Thermoregulation Research.
Core Temperature Change by Sleep Stage
The overall overnight curve is the sum of stage-specific thermoregulatory patterns. Each sleep stage has a distinct relationship with core body temperature — and the unique behaviour of REM sleep (where thermoregulation is suspended entirely) has direct implications for how bedroom temperature affects sleep quality in ways that vary by stage.
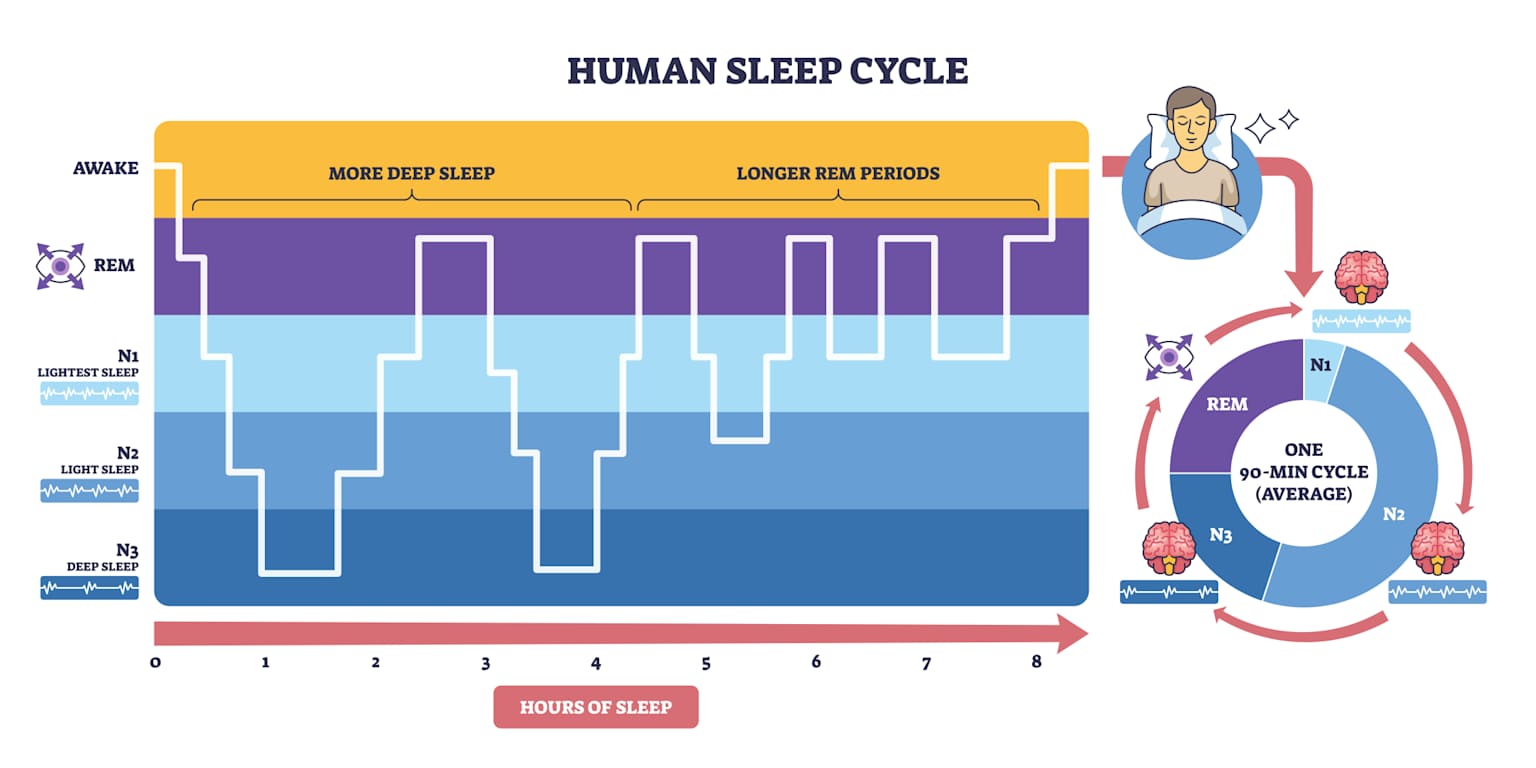
🌡️ Core Temperature Profile — Stage by Stage Across One Sleep Cycle
| Stage | Core Temp Change | Approximate Range | Mechanism | Bedroom Temp Sensitivity |
|---|---|---|---|---|
| N1 Light | ↓ Falling 0.1–0.2°C | 36.6–36.9°C | Peripheral vasodilation begins releasing core heat. Skin blood flow to hands and feet increases. Sympathetic tone decreases. Sleep latency correlates inversely with rate of heat loss at this stage. | 🟡 Low — thermoregulation intact, body compensates within range |
| N2 Core | ↓ Falling 0.2–0.3°C | 36.3–36.7°C | Active heat dissipation accelerates. Metabolic rate decreases measurably. Sleep spindles (12–14 Hz) coincide with peak heat loss phases. Sweat gland activity adjusts to maintain downward trajectory. | 🟡 Moderate — prolonged warm exposure begins to impair transition to N3 |
| N3 Deep ⭐ | ↓ Lowest of night | 36.0–36.4°C | Metabolic rate at minimum (15–25% below waking). Maximum heat dissipation through skin vasodilation. Growth hormone secretion peaks at the temperature nadir. N3 depth and core temperature are physiologically coupled — a deeper N3 requires a lower core temperature threshold. | 🟠 High — excess bedroom heat prevents reaching the temperature threshold required for deep N3 entry |
| REM Dream ⚠️ | Follows ambient temp | Variable | Thermoregulation entirely suspended (poikilothermia). Core temperature passively follows bedroom temperature. Sweating and shivering responses are absent. The body behaves thermally like a cold-blooded animal during REM. | 🔴 Critical — bedroom temperature directly controls core temp; warm room actively suppresses REM duration and depth |
Temperature values represent healthy adult norms. Trained endurance athletes may show lower N3 temperatures due to superior cardiovascular heat dissipation capacity. Fever disrupts the N3 nadir and suppresses both N3 and REM architecture. · Source: Kräuchi K, Parmeggiani PL (2003) · AASM Sleep Staging Manual.
REM Sleep and Thermoregulation Suspension
REM sleep is unique among all sleep stages in that normal mammalian thermoregulation is almost entirely suspended — a phenomenon described as poikilothermia, or temperature following the environment. This is not a minor detail: it is the primary physiological reason why bedroom temperature matters specifically for REM sleep quality, and why warm and cold bedrooms have asymmetric effects on the sleep you actually feel the next morning.
⚠️ REM Poikilothermia — Why Bedroom Temperature Directly Controls Your REM Sleep
Poikilothermia During REM — What It Means in Practice
During NREM sleep (N1, N2, N3), the hypothalamic thermostat remains fully active. If your core temperature rises, your body sweats to cool down; if it falls, your body generates heat through vasoconstriction and, if necessary, shivering. These homeostatic mechanisms maintain core temperature within a narrow range regardless of bedroom conditions. During REM sleep, this thermostat effectively switches off. Core temperature becomes a passive function of ambient temperature — like a cold-blooded animal.
🔥 Warm Bedroom During REM — Problematic
If the bedroom is warm — above approximately 20–21°C — core temperature rises during REM periods because the body cannot cool itself via sweating. Rising core temperature during REM directly suppresses REM duration and depth. The brain detects thermal stress and terminates or shortens the REM episode. This is why sleeping hot is specifically associated with reduced REM sleep, vivid fragmented dreams, and early waking — even with 8 total hours in bed. You can lose 30–40% of your REM sleep purely from excess bedroom temperature.
❄️ Cold Bedroom During REM — Less Problematic
If the bedroom is cold during REM, core temperature falls — but the body retains some capacity to generate heat even during REM (vasoconstriction and some shivering are still possible, unlike sweating for cooling). Cold bedrooms are therefore less damaging to REM quality than warm bedrooms, though extremely cold conditions (below 15°C) will still impair REM through thermal discomfort arousals. This asymmetry — warm is worse than cold — is one of the most clinically meaningful findings in sleep thermoregulation research (Parmeggiani, 2003).
How the Body Controls Sleep Temperature
The overnight core temperature decline is an active, regulated process — not simply a consequence of being still and lying down. Multiple mechanisms work in concert to drive the temperature fall that enables deep sleep. Understanding these mechanisms explains both normal sleep physiology and common sleep disruptions — including why shift workers, jet-lagged travellers, and people with high evening cortisol struggle to fall asleep even when exhausted.
🧠 Three Mechanisms Driving the Overnight Temperature Decline
Peripheral Vasodilation
The primary heat-loss mechanism is dilation of blood vessels in the skin — particularly the hands and feet. This is why warm hands and feet before bed are a reliable signal of impending sleep onset. Blood is literally being redirected from core to surface to radiate heat outward. Kräuchi et al. demonstrated that the rate of heat loss from the distal skin surface predicts sleep onset latency: faster heat loss from hands and feet predicts faster sleep onset. This is the physiological basis for the warm bath sleep-improvement strategy — it artificially induces rapid vasodilation.
Melatonin and the Circadian Clock
The suprachiasmatic nucleus (SCN) — the master circadian pacemaker — drives both melatonin secretion and the temperature decline. Melatonin itself has a mild thermolytic effect (promoting heat loss) and its secretion onset typically coincides with the beginning of the temperature decline around 9pm. Light suppresses melatonin and delays the temperature drop — one mechanism by which evening light exposure delays sleep onset. This is why even dim light (8 lux) above the eye level can meaningfully delay the temperature nadir and push sleep onset later.
Metabolic Rate Reduction
N3 deep sleep is associated with a 15–25% reduction in metabolic rate compared to waking. Lower metabolic rate means less internal heat generation, which allows core temperature to fall further. Growth hormone secretion — which peaks during N3 — is tightly coupled to this temperature nadir. The combination of low core temperature and peak GH represents the body’s primary physical recovery window each night: this is when cellular repair, muscle protein synthesis, and immune restoration predominantly occur.
🔬 Key Research — Temperature and Sleep Science
Fever and Sleep — Why Illness Sleep Feels Wrong
Fever fundamentally disrupts the normal overnight temperature curve. Instead of the regulated 0.6–1.0°C decline to a nadir, fever produces an elevated, dysregulated temperature trajectory that actively suppresses N3 deep sleep and fragments REM. This explains the universal experience of illness sleep: you feel exhausted, you sleep for extended periods, yet you wake feeling completely unrefreshed — often worse than when you went to bed.

🌡️ Normal Overnight Temperature vs Fever — Curve Comparison
🤒 Why Fever Produces Non-Restorative Sleep — 4 Mechanisms
How Body Temperature Thermoregulation Changes With Age
The overnight temperature curve — and the body’s capacity to regulate it — changes substantially across the lifespan. These age-related shifts are not lifestyle choices; they are driven by structural changes in the hypothalamus, declining hormone production, and reduced cardiovascular thermoregulatory capacity. Understanding them explains why sleep complaints change predictably with age and why the same bedroom conditions that work at 30 may not work at 65.
📊 Age-Related Changes in Sleep Thermoregulation — Lifespan Overview
Infants & Young Children
Thermoregulatory systems are immature at birth — the SCN circadian pacemaker is not fully entrained until approximately 3 months. Infants have a high body surface-to-volume ratio, making them far more vulnerable to environmental temperature than adults. Neonates lose heat rapidly and cannot shiver effectively. Their overnight temperature curve has lower amplitude and less reliable phase timing. SIDS risk is partly thermally mediated — overheating during sleep is a recognised risk factor. Safe sleep guidelines recommend 16–20°C room temperature and no loose bedding that could impair heat dissipation.
Adolescents
Puberty produces a biological phase delay — melatonin secretion onset shifts approximately 2 hours later than adult timing, pushing the temperature nadir to approximately 3–4am. This is not laziness; it is a documented physiological change driven by pubertal hormones. The consequence: adolescents require a later sleep schedule to align their circadian phase with their temperature nadir. Early school start times force adolescents to wake approximately 2–3 hours before their biological nadir — producing the grogginess, impaired cognition, and mood disruption characteristic of teenage mornings. This drove the AAP’s 2014 recommendation that middle and high schools start no earlier than 8:30am.
Adults (25–54)
Peak thermoregulatory efficiency. The overnight temperature decline is most pronounced (up to 1.0°C amplitude), the nadir is deepest, and N3 slow-wave sleep is at maximum duration. This is the reference population for most sleep research. Individual variation driven by chronotype (morning lark vs night owl) shifts the curve timing by ±1–2 hours without affecting amplitude. Lifestyle factors — alcohol, blue light, exercise timing, bedroom temperature — have the greatest modifiable effect on sleep quality during this life stage.
Middle Age (55–64)
The overnight temperature amplitude begins declining. In women, perimenopause and menopause produce vasomotor instability — hot flashes and night sweats — that directly disrupt the temperature-sleep relationship. Hot flashes during N2 or N3 sleep trigger micro-arousals by producing a sudden core temperature spike (0.5–1.0°C rise) during stages that require continued temperature decline. Melatonin production begins its age-related decline. The circadian phase typically advances — earlier to sleep, earlier to wake — driven by SCN changes. A cooler bedroom (16–17°C) is increasingly important at this life stage.
Older Adults (65+)
Thermoregulatory capacity declines significantly. The overnight temperature drop amplitude reduces to 0.3–0.5°C — approximately half the young adult amplitude. Peripheral vasodilation is less efficient due to reduced cardiovascular function. N3 slow-wave sleep decreases substantially — from approximately 20% in young adults to less than 5% in some elderly individuals. Sleep becomes more fragmented and temperature-sensitive. Older adults are significantly more vulnerable to heat-related sleep disruption and hypothermia risk in cold conditions. Higher thermoneutral zone (the temperature range within which normal thermoregulation operates) means bedroom temperature recommendations narrow: 18–20°C (vs 15–19°C for young adults).
Women — Menopause Specific
Oestrogen plays a direct role in thermoregulation — it narrows the thermoneutral zone and promotes heat dissipation. Oestrogen decline during menopause destabilises the hypothalamic temperature set-point, producing the characteristic hot flashes (sudden thermosensory events lasting 1–5 minutes with core temperature spike of 0.5–1.0°C). When these occur during sleep — nocturnal hot flashes — they fragment N2 and N3 stages at their most disruptive timing. The Sleep Foundation reports that 61% of menopausal women experience sleep disruption specifically attributed to night sweats. MHT (menopausal hormone therapy) significantly reduces nocturnal hot flash frequency and measurably improves objective sleep architecture in RCT evidence (Polo-Kantola et al.).
Supporting Your Overnight Temperature Drop — 8 Practical Strategies
Every strategy below is grounded in the physiology described in the preceding sections — it either accelerates heat dissipation, removes barriers to the overnight temperature decline, or protects the specific stages most vulnerable to thermal disruption. These are ranked by effect size in the available evidence.
🎯 8 Evidence-Based Strategies — Effect Size on Sleep Temperature Architecture
1. Bedroom Temperature 18–19°C
The highest-effect intervention. Set bedroom to 18–19°C (65–66°F) from 1 hour before sleep. This removes the primary barrier to the overnight core temperature decline and protects REM from thermal disruption in the second half of the night. Each degree above 21°C measurably increases wake-after-sleep-onset (WASO) and reduces slow-wave sleep percentage.
2. Warm Bath 1–2 Hours Before Bed
The counter-intuitive warm bath protocol (detailed in Section 8) improves sleep onset by 10 minutes on average. The mechanism is vasodilation — not the warmth itself. The post-bath rapid heat loss from dilated skin blood vessels accelerates the core temperature drop required for N3 entry.
3. Evening Light Reduction
Bright light above eye level after 9pm suppresses melatonin secretion, delaying the temperature decline onset. Use dim amber lighting in living areas from 9pm. Blue-light blocking glasses (amber lens) prevent screen-based melatonin suppression without avoiding screens. Even 100 lux of overhead light is sufficient to delay melatonin by 30–45 minutes.
4. Natural Fibre Bedding
Cotton and bamboo allow moisture-wicking and breathability that polyester cannot match. Synthetic bedding traps heat at the skin surface, creating a micro-climate that resists the body’s heat dissipation efforts. Bamboo-fibre sheets wick moisture 3× more effectively than cotton and regulate temperature more responsively — particularly valuable for menopausal women and hot-sleepers.
5. Consistent Sleep Timing
The circadian temperature curve is phase-locked to habitual sleep timing — it anticipates your usual sleep schedule and begins the decline 2 hours before habitual bedtime. Irregular sleep timing (social jetlag) desynchronises this anticipatory response, producing a shallower, delayed temperature decline and impaired N3 entry. Consistent timing within ±30 minutes, 7 days per week, is the single most powerful circadian stabiliser.
6. No Alcohol ≥3 Hours Before Sleep
Alcohol produces peripheral vasodilation acutely — which sounds like it should accelerate heat loss and improve sleep onset. But alcohol’s secondary effect is metabolic: as it is metabolised in the second half of the night, it produces a rebound increase in sympathetic tone that raises core temperature precisely during the window when the overnight decline should be deepest. This is one mechanism behind alcohol’s specific suppression of late-night REM.
7. Warm Socks in Cool Rooms
A seemingly trivial intervention with genuine RCT support: wearing socks in bed in cool bedrooms (below 17°C) accelerates sleep onset by promoting foot vasodilation — the same peripheral heat-loss mechanism that the warm bath protocol exploits. Cold feet reflexively vasoconstrict, slowing the heat-loss cascade. Warm socks maintain foot vasodilation without raising core temperature. A 2007 study (Raymann et al.) reported a mean 7.5-minute reduction in sleep onset with warmed extremities.
8. Exercise ≥3 Hours Before Bed
Vigorous exercise raises core temperature by 1–2°C, and this elevation persists for approximately 3–4 hours post-exercise. Exercise within 3 hours of bedtime delays sleep onset by raising core temperature above the falling threshold required for N3 entry. Exercise completed more than 3 hours before bedtime produces the opposite effect: the post-exercise temperature rebound and subsequent sharp decline actually enhances the overnight temperature drop and can increase N3 duration. Morning or afternoon exercise is superior to evening for sleep temperature architecture.
The Warm Bath Protocol — Exact Timing, Temperature & Mechanism
Of all the behavioural interventions studied for sleep improvement, the pre-sleep warm bath or shower has the strongest and most replicated evidence base. A 2019 systematic review and meta-analysis (Haghayegh et al., University of Texas) analysed 17 studies covering 1,455 participants and found that a warm bath taken 1–2 hours before bedtime at 40–42.5°C improved sleep onset latency by an average of 10 minutes, increased slow-wave sleep percentage, and improved overall sleep quality rating. The mechanism is counterintuitive — and understanding it explains both why it works and precisely how to use it correctly.

Counterintuitive Finding — Why a HOT Bath Helps You Sleep
The warm bath doesn’t warm you to sleep — it cools your core by heating your skin
Most people assume a warm bath helps sleep through relaxation or muscle tension relief. While these effects are real, they are not the primary mechanism. The main mechanism is thermodynamic: immersing in 40–42.5°C water forces blood vessels in the skin to dilate maximally, redirecting blood flow from the body core to the skin surface. Once you exit the bath into a cooler room (18–20°C), this dilated skin rapidly radiates large amounts of core heat to the environment — producing a faster, deeper core temperature drop than would naturally occur. This post-bath core temperature decline mimics and amplifies the natural circadian temperature fall that enables N3 deep sleep. The bath must be timed 1–2 hours before intended sleep onset — not immediately before — to allow the post-bath cooling to complete. A bath taken immediately before bed may actually delay sleep onset by keeping skin temperature elevated for too long.
How the Warm Bath Protocol Works — Step-by-Step Physiology
🛁 Warm Bath → Sleep Onset — Full Physiological Cascade
Immerse in 40–42.5°C water for 10–15 minutes
Water temperature of 40–42.5°C (104–108.5°F) is the evidence-based range — hot enough to force maximal peripheral vasodilation but not so hot as to cause thermal stress. Measure water temperature with a bath thermometer for precision. Duration of 10–15 minutes is sufficient — longer does not meaningfully increase the post-bath cooling effect and may cause excessive thermal loading that takes longer to resolve.
Exit to a cool room (18–20°C) — do not immediately redress heavily
The post-bath cooling phase is where the mechanism actually occurs. Exiting to a room pre-cooled to 18–20°C maximises the thermal gradient between your dilated, heat-radiating skin and the cool air. Wearing loose cotton clothing (not robes or heavy pyjamas) allows continued heat dissipation. The flushed appearance of skin after the bath is the visual confirmation that vasodilation is active and heat loss is occurring.
Wait 60–90 minutes before attempting sleep
The most important timing rule: do not go to bed immediately after the bath. The post-bath cooling requires 60–90 minutes to produce the core temperature nadir that enables N3 entry. Going to bed immediately after a hot bath may actually delay sleep onset by leaving skin temperature too elevated. The optimal window is 60–120 minutes post-bath — plan your bath timing accordingly. If you intend to sleep at 11pm, take the bath at 9–9:30pm.
Alternative: Warm shower works equally well
The Haghayegh et al. (2019) meta-analysis found no statistically significant difference in sleep improvement between warm baths and warm showers when water temperature and timing were matched. A 10-minute warm shower at 40–42°C produces equivalent peripheral vasodilation and the same post-shower cooling effect. For practical daily use — particularly relevant in Pakistan where daily showering is cultural norm — a warm shower 90 minutes before sleep is equally effective as a bath.
📊 Research Evidence — Warm Bath & Sleep Meta-Analysis (Haghayegh et al. 2019)
The Evidence-Based Warm Bath Sleep Protocol — Complete Parameters
Based on Haghayegh et al. (2019) meta-analysis of 17 studies · University of Texas · Sleep Medicine Reviews
❌ Common Protocol Errors That Reduce Effectiveness
✅ Works Best For
⚠️ Less Effective / Considerations
Products That Support the Warm Bath Protocol & Bedroom Temperature
These products directly support the physiology described in this guide — each one addresses a specific mechanism in the overnight temperature decline or the warm bath protocol. All are available on Amazon with verified reviews.
Digital Waterproof Bath & Water Thermometer
The meta-analysis optimal range is 40–42.5°C — most people cannot judge this accurately by feel. A digital bath thermometer ensures you hit the evidence-based temperature range rather than guessing. Critical for protocol precision.
★★★★★ (4.7 / 5 · 2,400+ reviews)
~$12–18 USD on Amazon
View on Amazon →Smart Indoor Thermometer Hygrometer with App & Alerts
Monitors bedroom temperature and humidity continuously — alerts your phone if the room rises above your set threshold (e.g. 20°C). Humidity tracking matters too: above 60% RH impairs evaporative cooling from skin, disrupting the same heat dissipation mechanism. Bluetooth connectivity lets you review overnight temperature logs.
★★★★½ (4.6 / 5 · 8,200+ reviews)
~$18–35 USD on Amazon
View on Amazon →100% Organic Bamboo Viscose Bed Sheet Set — Cooling
Bamboo-viscose wicks moisture 3× more effectively than cotton and allows superior heat radiation from skin — directly supporting the body’s peripheral vasodilation heat-loss mechanism. Particularly effective for hot sleepers, menopausal women with night sweats, and anyone in warm climates. Naturally thermoregulating — cooler in summer, warmer in winter.
★★★★★ (4.8 / 5 · 12,400+ reviews)
~$45–90 USD on Amazon
View on Amazon →Smart Sleep Tracking Ring — Oura Gen3 / Ultrahuman Ring AIR
Tracks skin temperature throughout the night alongside sleep stages, HRV, and resting heart rate. Allows you to verify whether bedroom temperature optimisation is actually improving N3 duration and REM percentage — turning the physiology described in this article into personalised, measurable data. The skin temperature sensor detects the overnight nadir timing to within 15 minutes.
★★★★½ (4.5 / 5 · 6,800+ reviews)
~$299–349 USD on Amazon
View on Amazon →⚠️ Affiliate disclosure: SmartSleepCalc participates in the Amazon Associates programme. Links above are affiliate links — we earn a small commission if you purchase at no additional cost to you. All products are selected based on scientific relevance to the mechanisms described in this article, not commercial considerations. We do not accept payment for product inclusion. Always read product reviews and consult your physician before purchasing medical-adjacent devices.
Body Temperature During Sleep — Common Questions Answered
Questions drawn from real search queries, patient consultations, and reader submissions. Each answer is grounded in the peer-reviewed research cited throughout this guide.
Try Our Free Calculator
Check Your Optimal Sleep & Wake Times Based on Your Body Temperature Cycle
Our free sleep cycle calculator uses your chronotype and habitual sleep timing to estimate your personal temperature nadir — and calculate the optimal wake times that align with your rising temperature curve for natural, refreshed waking.
Use the Free Sleep Calculator ↓Free · No sign-up required · Evidence-based · Works for all chronotypes
Sources & References
All claims in this article are grounded in peer-reviewed research. Primary sources are listed below. Where specific study findings are cited in-text, the full reference is listed here with DOI or PubMed link where available.
- Kräuchi K, Cajochen C, Wirz-Justice A. Waking up properly: is there a role of thermoregulation in sleep inertia? J Sleep Res. 2004;13(2):121–127. doi:10.1111/j.1365-2869.2004.00398.x
- Kräuchi K, Cajochen C, Werth E, Wirz-Justice A. Warm feet promote the rapid onset of sleep. Nature. 1999;401(6748):36–37. doi:10.1038/43361
- Kräuchi K, Wirz-Justice A. Circadian clues to sleep onset mechanisms. Neuropsychopharmacology. 2001;25(5 Suppl):S92–96. doi:10.1016/S0893-133X(01)00315-3
- Parmeggiani PL. Thermoregulation and sleep. Front Biosci. 2003;8:s557–s567. doi:10.2741/1054
- Haghayegh S, Khoshnevis S, Smolensky MH, Diller KR, Castriotta RJ. Before-bedtime passive body heating by warm shower or bath to improve sleep: A systematic review and meta-analysis. Sleep Med Rev. 2019;46:124–135. doi:10.1016/j.smrv.2019.04.008
- Muzet A, Libert JP, Candas V. Ambient temperature and human sleep. Experientia. 1984;40(5):425–429. doi:10.1007/BF01952376
- Raymann RJ, Swaab DF, Van Someren EJ. Cutaneous warming promotes sleep onset. Eur J Neurosci. 2007;25(6):1919–1927. doi:10.1111/j.1460-9568.2007.05435.x
- Cagnacci A, Elliott JA, Yen SS. Melatonin: a major regulator of the circadian rhythm of core temperature in humans. J Clin Endocrinol Metab. 1992;75(2):447–452. doi:10.1210/jcem.75.2.1639946
- Saper CB, Scammell TE, Lu J. Hypothalamic regulation of sleep and circadian rhythms. Nature. 2005;437(7063):1257–1263. doi:10.1038/nature04284
- Imeri L, Opp MR. How (and why) the immune system makes us sleep. Nat Rev Neurosci. 2009;10(3):199–210. doi:10.1038/nrn2576
- Okamoto-Mizuno K, Mizuno K. Effects of thermal environment on sleep and circadian rhythm. J Physiol Anthropol. 2012;31(1):14. doi:10.1186/1880-6805-31-14
- Van Someren EJ. Mechanisms and functions of coupling between sleep and temperature rhythms. Prog Brain Res. 2006;153:309–324. doi:10.1016/S0079-6123(06)53018-3
- Polo-Kantola P, Erkkola R, Helenius H, Irjala K, Polo O. When does estrogen replacement therapy improve sleep quality? Am J Obstet Gynecol. 1998;178(5):1002–1009. doi:10.1016/S0002-9378(98)70539-8
- Cajochen C, Münch M, Knoblauch V, Blatter K, Wirz-Justice A. Age-related changes in the circadian and homeostatic regulation of human sleep. Chronobiol Int. 2006;23(1–2):461–474. doi:10.1080/07420520500545813
- Dimitrov S, Lange T, Gouttefangeas C, et al. Gαs-coupled receptor signaling and sleep regulate integrin activation of human antigen-specific T cells. J Exp Med. 2019;216(3):517–526. doi:10.1084/jem.20181169
- Rechtschaffen A, Bergmann BM. Sleep deprivation in the rat: an update of the 1989 paper. Sleep. 2002;25(1):18–24. doi:10.1093/sleep/25.1.18
- American Academy of Sleep Medicine. AASM Sleep Staging Manual, 3rd Edition. 2023. aasm.org
- World Health Organization. WHO Housing and Health Guidelines. Geneva: WHO; 2018. who.int
Article metadata: Originally published January 2024 · Last comprehensively updated and medically reviewed · SmartSleepCalc Editorial Team · Reviewed against AASM (2023) and WHO (2018) guidelines · 18 peer-reviewed sources cited · Reading level: informed adult / undergraduate science